
 Excess of cartilage resection from the tip and from the dorsum. Secondary Rhinoplasty, reconstruction with cartilage retrieved from the ear cartilage. Pre and post-operative photos.
Excess of cartilage resection from the tip and from the dorsum. Secondary Rhinoplasty, reconstruction with cartilage retrieved from the ear cartilage. Pre and post-operative photos.
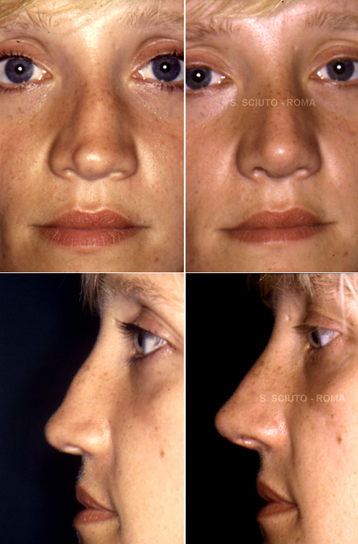
 Shortening an over-projected tip is certainly a complex procedure and any attempt to perform this by over-correcting the dorsum results in a seriously deformed and almost irreparably damaged nose. In this case, revision has obtained a natural and pleasant shape by balancing the shortening of the tip with moderate lengthening of the dorsum. Pre and post-operative photos
Shortening an over-projected tip is certainly a complex procedure and any attempt to perform this by over-correcting the dorsum results in a seriously deformed and almost irreparably damaged nose. In this case, revision has obtained a natural and pleasant shape by balancing the shortening of the tip with moderate lengthening of the dorsum. Pre and post-operative photos
 Correction of the nasal septum is an integral part of effective rhinoplasty as regards not only functional but also aesthetic results. Narrowing the nose without correcting the septum makes deviation of the latter still more evident and leads to a worsening of respiration. Pre and post-operative photos.
Correction of the nasal septum is an integral part of effective rhinoplasty as regards not only functional but also aesthetic results. Narrowing the nose without correcting the septum makes deviation of the latter still more evident and leads to a worsening of respiration. Pre and post-operative photos.
 Excess of cartilage resection. Secondary Rhinoplasty, reconstruction of the tip with cartilage retrieved from the nasal septum. Pre and post-operative photos.
Excess of cartilage resection. Secondary Rhinoplasty, reconstruction of the tip with cartilage retrieved from the nasal septum. Pre and post-operative photos.
 Tertiary Rhinoplasty (already 2 previous surgeries): reconstruction with cartilage retrieved from the rib. Pre and post-operative photos.
Tertiary Rhinoplasty (already 2 previous surgeries): reconstruction with cartilage retrieved from the rib. Pre and post-operative photos.
 Secondary rhinoplasty: symmetrization of the tip cartilages and dorsal trimming. Pre and post-operative photos.
Secondary rhinoplasty: symmetrization of the tip cartilages and dorsal trimming. Pre and post-operative photos.
The secondary rhinoplasty: when the surgery was unsuccessful
Around 20,000 rhinoplasty operations are carried out every year in Italy and in most cases with full satisfaction of the patient. However the vast diffusion and popularity of this surgery means that the number of those who are not completely happy with their "new nose" is unfortunately elevated. Consequently there is an increase in demand for secondary rhinoplasty.
What causes an unsuccessful rhinoplasty?
It is not always the fault of the surgeon.
The nose is a complex organ with many functions: smell, it heats the air, filters it, humidifies it. When one intervenes in the shape of the nose all these functions must be considered, as well as the recovery process that is never the same in any patient and is often unforeseeable: the cartilage can bend, the bones can knit irregularly, the swelling can persist for long periods and the final result can vary from person to person.
Bad post-operative scarring most frequently causes dissatisfaction or the typical "nose job" look that it is due, generally, to excessive removal of bone or cartilage.
Those who feel the necessity of a secondary rhinoplasty are a most always patients that never liked their "new nose" and at the same time complain of persistent respiration difficulty. .
Is secondary rhinoplasty more difficult?
It must be accepted that most of the time the objective of a secondary rhinoplasty is improvement and not perfection. It is however undeniable that operating for the second time presents greater difficulties compared to a nose never operated on before.
In a patient that has never had surgery the different nasal tissues are layered naturally: the surgeon can easily separate the various layers to reach the structures on which to operate. But when the nose has already been operated on these layers no longer exist, and therefore the surgery is more difficult: it is as if someone put glue in the nose to join the skin to the bones and the cartilage underneath. This scar tissue (the glue) is very resistant and must be dealt with in a cautious and shrewd manner to avoid further damage. Moreover it can prevent achievement, especially at the level of the nasal tip, of definition and desired thinness.
If the defect is a residual hump, or an excessive irregularity of the bridge, the correction is easier. On the contrary it is much more difficult when dealing with a nose that has had too much removed: in nasal surgery it is easier to remove than to add.
In other words when the nose is too small, too short, too turned up, or pinched, secondary rhinoplasty is more difficult.
These are the cases in which the structures removed must be replaced with cartilage or bony grafts (always from the same patient). These grafts must be modeled and fixed in such a way as to give a pleasing shape to the nose and at the same time to restore correct functionality.
In some cases the damage is so great it requires the use of multiple grafts: autologous grafts are always used, that is, harvested from the same patient in separate procedures. Generally the main source for grafts is the nasal septum, but when, like with patients already operated on 3,4,5 or more times, the septum is completely lacking it is necessary to resort to other sites. The cartilage of the ear is first choice: it is retrieved through a small incision hidden behind the ear and its absence does not create any change in the shape of the auricular pavilion.
In certain cases it is necessary, in order to reconstruct the missing nasal structures, to resort to rib cartilage that is retrieved through a small incision in the chest.
What results do a secondary rhinoplasty give?
In spite of the technical difficulties of the surgery, reserved only for more expert surgeons, the majority of patients gain advantage from revision surgery, especially those with realistic expectations. Serious surgeons do not operate if they are not convinced that improvement is possible, but in many cases perfection cannot be guaranteed.
How to recognize an expert surgeon?
A surgeon who carries out 1 or 2 primary rhinoplasty surgeries a month is not a surgeon indicated for secondary rhinoplasty. Experience from performing a great number of nasal surgical procedures is necessary: today in Italy there are few surgeons who operate on more than 50 noses a year, just as worldwide there are few who operate on more than 100.
The "french" nose
 This young lady was operated on approximately 10 years previously.
This young lady was operated on approximately 10 years previously.
The initial result seemed pretty but as time gone on appeared more and more displeasing being too unnatural and artificial. The appearance was that of the classic "nose job". Her wish was to return to having a natural nose, straight, and in harmony with her face. The surgery had to succeed therefore in carrying out two fundamental corrections: first to correct the profile of the over-flattened bridge of the nose. This was achieved with grafts of cartilage taken from the patient's septum, fortunately still intact.
The second correction was much more difficult than the first: it was necessary to rotate the tip downwards to correct the exagerated "turned-up" appearance of the nose.
An extension graft was arranged in such a way to push the alar cartilages of the tip downwards. The appearance achieved is that of a beautiful nose, without excesses, adapted to the face and "absolutely natural".
A complex secondary rhinoplasty
Female, 24 years old, already operated on 3 times: the first an unsuccessful rhinoplasty, then two subsequent attempts to improve the original surgery, also unsuccessful. The structures that supported the nose, in particular the cartilages, appeared irreparably damaged: the nose was supported only by amorphous scar tissue that gave neither support nor definition to the tip, and had become shapeless. The bridge was too carved resulting in a "saddle nose". The nose had a negative effect on her appearance.

The entire structure of the nose had to be reconstructed with grafts: but which?
A malleable but at the same time rigid material was required, otherwise in the post-operative scarring contraction it would have folded or moved ruining the result. Moreover an abundant amount was needed, in order to reconstruct nearly all of the nasal structures.
The logical choice was rib cartilage from the patient herself: abundant, rigid, malleable, and above all perfectly biocompatible. The photos before and approximately 10 months after the secondary rhinoplasty surgery: even though the swelling will go down a little more the result can be considered definitive and stable.